Acne surgery is the manual removal of comedones and the drainage of pustules and cysts. When done correctly, acne surgery speeds resolution and rapidly enhances cosmetic appearance. Three instruments are used: the round loop comedone extractor; the oval loop acne extractor, or the Schamberg extractor; and the no. 11 pointed-tip scalpel blade.
 COMEDONES
COMEDONES
 COMEDONES
COMEDONESRemoval of open comedones (blackheads) enhances the patient’s appearance and discourages self-manipulation. By use of either type of extractor, most comedones can easily be expressed with uniform, smooth pressure.
Lesions that offer resistance are loosened and sometimes disengaged by inserting the point of a no. 11 blade into the blackhead and elevating. The orifi ce of the closed comedone must be enlarged before pressure can be applied. Following the angle of the follicle, the scalpel point is inserted with the sharp edge up approximately 1 mm into the tiny orifi ce. The blade is drawn slightly forward and up, then pressure is applied with the extractor to remove the sometimes surprisingly large quantity of soft, white material. Macrocomedones (whiteheads, microcystic acne) can also be treated with light cautery.
PUSTULES AND CYSTS
After the head of the white pustule is nicked with the no. 11 blade, pustules are easily drained by pressing the material with the acne extractor. Cysts are preferably managed by intralesional injection because incision and drainage may cause scarring. Pustules and cysts that have a thin, effaced roof in which fluid contents are easily felt are drained through a small incision by manual pressure. To prevent scarring, a short incision (approximately 3 mm) should be made.
After drainage, a no. 1 curette may be inserted through the incision on the cyst to dislodge chunks of necrotic tissue.
SCAR REVISION
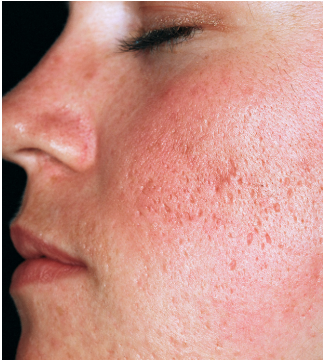
Many patients are very self-conscious about the pitted and crater like scars that remain as a permanent record of previous inflammation. Some people will endure any procedure and spare no expense to rid themselves of the most minute scar.
Three scar types: icepick, rolling, and boxcar can form. Treatments include punch excision, punch elevation, subcutaneous incision (subcision), scar excision, and laser skin resurfacing. A dermatologic or plastic surgeon is best equipped to perform such procedures.
Generally, it is advisable to wait until disease activity has been low or absent for several months. Scars improve as they atrophy. The color contrast is often the most troublesome aspect of acne. Infl amed lesions may leave a flat or depressed red scar that is so obvious patients mistake the mark for an active lesion. The color will fade and approach skin tones in 4 to 12 months



